
In a 3/6/16 Facebook post, I listed six “not-so-sudden warning signs of sudden cardiac arrest” that Los Angeles medical researchers had identified in a study I read about in the newsletter “Health After 50” (vol. 28, issue 2, April 2016). They are:
1) Chest pain (angina) or pressure
2) Shortness of breath (dyspnea)
3) Racing heartbeat
4) Fainting (preceded by lightheadedness or dizziness)
5) Unusual abdominal or back pain
6) Flulike symptoms, such as nausea and vomiting
According to a summary of the study, which was published in “Annals of Internal Medicine” (“Annals”) in January, these signs may occur weeks before a stricken person’s heart suddenly stops beating, thus opening a prevention window that has not previously been recognized.
Articles in “Annals,” which is the journal of the American College of Physicians, a membership organization of internal-medicine physicians, are accessible online only by subscribers, of which I am not one. I did some research on this study, however, and pass along to you what I could glean, including the citations for both the “Annals” report:
Eloi Marijon, Audrey Uy-Evanado, et al, “Warning Symptoms May Prevent Some Cases of Sudden Cardiac Arrest,” Ann. Intern. Med. 2016, 164(1): 1-22. (I’ll be looking it up in a medical library soon.)
And another “Annals” article related to the study, which focuses on disparities in the life-and-death efficiency of communities’ and hospitals’ emergency-response systems and demands improvement in care:
Thomas Rea and Mickey Eisenberg, “Sudden Cardiac Arrest: A Call to Action From the Institute of Medicine,” Ann. Intern. Med. 2015, 163(10): 794-95. (This can be accessed at http://annals.org/article.aspx?articleid=2434627.)
Researchers at Cedars-Sinai Medical Center in L.A. collected data on 839 middle-aged people (ages 35 to 65) who had suffered sudden cardiac arrest (SCA) in a Northwest U.S. city over a period of years. They found that a majority of these patients had experienced warning symptoms in the four weeks before their heart stoppage, and, of those who did, nearly all experienced symptoms again in the 24 hours before SCA. The most common warning symptoms were chest pain and shortness of breath.
Sudden cardiac arrest—stoppage of the heart—results when the heart’s electrical system malfunctions. In contrast, a heart “attack” occurs when the heart’s circulation is impaired or obstructed.
SCA most commonly happens when the heart’s electricity is interrupted, such as by an irregular heartbeat or an arrhythmia that triggers ventricular fibrillation. When the heart’s ventricles, which are the two muscles (chambers) responsible for its contractions, fibrillate, they quiver instead of pump blood through it. Once the heart stops beating, blood stops flowing to the brain and other vital organs; the patient loses consciousness within seconds to minutes; and death occurs within 10 minutes.
According to “Health After 50,” which is an excellent resource affiliated with “Scientific American” and overseen by a medical board of editors from Johns Hopkins, the risk of SCA-related disability, such as brain injury, increases for each minute a person is not treated.” Even with survival, a patient “may need ongoing care for heart, lung or neurological problems,” it reports.
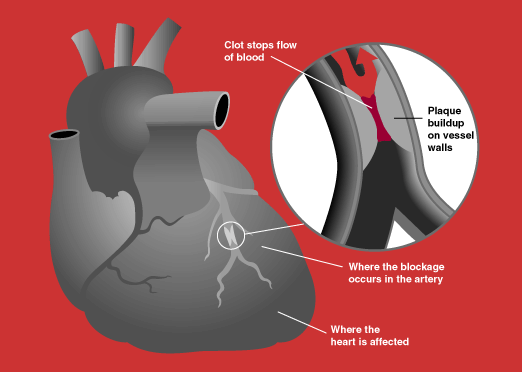
In “Our Parents in Crisis,” I take pains to explain what a heart “attack” is and to distinguish it from cardiac arrest. A heart attack is a myocardial infarction or MI, myocardial connoting heart muscle and infarction meaning tissue death. An MI occurs when a narrowing or blockage in one of the heart’s arteries obstructs the flow of oxygen-rich blood to an area of the heart, and the deprived tissue is injured or dies. Symptoms of an MI, according to “Health After 50,” include “chest or upper-body pain, fatigue, weakness, nausea, and shortness of breath”—symptoms similar to those for sudden cardiac arrest. Sufferers typically have a pulse and do not lose consciousness unless the MI causes cardiac arrest.
Besides an arrhythmia or an MI, some other causes of electrical malfunction that can precipitate SCA, according to “Health After 50,” include very low blood levels of magnesium or potassium (these are electrolytes); illegal or recreational drug use, such as cocaine or amphetamines; a structural heart problem caused by an enlarged heart (cardiomyopathy), advanced heart disease, or a heart infection; and, “extreme physical stress, including a severe loss of blood or lack of oxygen, intense physical activity that causes a surge in adrenaline, near drowning or electrocution, or other types of trauma.”
The National Academy of Medicine reports that fewer than 6 percent of all people who experience sudden cardiac arrest outside of a hospital survive, and only 24 percent of patients who suffer SCA in a hospital are saved. There is, thus, great medical incentive to be able to identify people who may be so stricken and to take measures to prevent their sudden deaths.
The mean age of the 839 patients whom the Cedars-Sinai researchers assessed was 52.6 years. Seventy-five percent of them were men. I was not able to read the description of their methodology. All I know is that they principally relied upon medical and emergency-response-team records and the recollections of families and friends of patients.
“Information was not available for about one quarter of the patients,” according to a free “Annals” summary written for patients. “For [others,] the experience of almost dying may have made it difficult for them to report accurately.” Despite these limitations, and others, it’s fair to say that the data may be useful in learning how to identify people who soon may experience sudden cardiac arrest.
Fifty percent of the men and 53 percent of the women in the study reportedly had warning symptoms in the four weeks before their heart stoppage. Of these patients, 93 percent experienced symptoms again in the 24 hours before the cardiac arrest, but only 19 percent of them called 911. Those who did were more likely to be older, to have a history of heart disease, or to be in continuous chest pain. Of the 19 percent who called for emergency assistance, 32 percent survived. Only 6 percent of those who did not call 911 survived.
According to “Health After 50,” cardiopulmonary resuscitation (CPR) by fast-acting bystanders and the use of an automated external defibrillator device (AED) to restore heart rhythm” were “associated with a better chance of survival.” CPR instruction is not typically part of Americans’ education. I took a CPR course 30 years ago and learned a technique that is no longer recommended, but I could get by. Mea culpa.
In evaluating the patients, the researchers discerned an important difference between men and women, which has been described elsewhere. Although chest pain was the most common symptom among all of the patients, it was more common among the men, 54 percent of whom had chest pain as compared with only 24 percent of the women. Women were more likely to experience dypsnea.
The message I take away from this study, as a patient, is that if I experience any of these symptoms, for no previously diagnosed reason, I should call 911 and, if I survive long enough, be seen in a hospital emergency department. I should not ignore or minimize my symptoms. Having been in many EDs with my parents, however, I know that medical care varies considerably from hospital to hospital, and the message should not end there. (See reference to disparities above.)
Coincidentally, The Washington Post’s March 8, 2016 “Health and Science” section featured a compelling first-person story by a 46-year-old woman who did not die because her husband insisted that her vomiting and “weird” and “kind of funny” feelings could be symptoms of more than a virus.
“You could be having a heart attack,” Nashville attorney Sue Palmer’s husband, Tim, told her. Tim’s father had died at age 64 from an MI, so he knew to be alert for non-classical symptoms. Sue wanted to go back to bed and wait out this “24-hour bug.”
Sue Palmer had the good fortune to be able to go to the emergency department of Vanderbilt University Medical Center, where a top-flight medical team took her comment, “My husband thinks I may be having a heart attack,” seriously. The team fast-tracked her examination and did not send her home after her first EKG showed no abnormalities. A second EKG taken 10 minutes after the first was different, and soon, Palmer was in the catheterization lab, where a superb interventional cardiologist determined that she had 100 percent blockage of her right coronary artery and 70 percent of her left anterior descending artery (LAD), which branches off of the left coronary artery. (An MI due to LAD blockage is known as “the widowmaker.”)
The cardiologist “literally stopped the heart attack while it was happening,” Palmer writes,“ by suctioning out a blood clot and putting two stents into my right coronary artery through a tiny hole he pierced in my right wrist.” See The Washington Post, “She Thought It Was Only a 24-Hour Bug. What She Really Had Almost Killed Her” at https://www.wshingtonpost.com/national/health-science/she-thought-it-was-only-a-24-hour-bug-what-she-really-had-almost-killed-her/2016/03/07/32e6cbfa-c5f5-11e5-a4aa-f25866ba0dc6_story.html.
Palmer had neither chest pain/pressure nor any personal or family history of heart disease. She didn’t smoke, and she wasn’t overweight. She exercised regularly and ate a healthy diet. Her cholesterol and blood pressure were normal. Nonetheless, plaque had ruptured in the wall of her right coronary artery, she reports, causing a clot to form.
Palmer’s message is the same as the one that emerges from the Cedars-Sinai study: Don’t ignore symptoms. Get yourself checked out. It can happen to you.
To this advice, I would add, that once you get to the emergency department, insist upon an EKG. If the electrocardiogram shows your heart is in normal sinus rhythm, as Palmer’s first EKG did, ask for a repeat EKG. In order to be safe, not sorry, you may need to ignore local ED physicians’ minimizing of your symptoms and advocate for further medical intervention. If you happen to be four weeks or two hours removed from a sudden cardiac arrest, prevention and survival depend not only on your awareness, but on the care and treatment you receive.
Ann, 3/10/16
The “widowmaker”
