FACT: Being overweight can prevent your body from making insulin properly.
FACT: Increased fat makes it harder for your body to use insulin properly, too.
FACT: An increase of visceral fat (i.e., belly fat) is particularly damaging to insulin function.
**
In the 1980s, endocrinologist and diabetes specialist Dr. Stephen Clement “rarely” saw a patient with Type 2 diabetes mellitus (DM) in the clinic. Today, the Georgetown University medical professor said he sees patients with this form of the blood-sugar disorder, formerly known as adult-onset diabetes, all of the time—including teenagers and children. The numbers, he told my mini-medical school class last week, are staggering. I was struck by the fact that Type 2 DM was rare in a decade that doesn’t seem that long ago to me.
Clement has no problem identifying the primary cause of the explosion in Type 2 diabetes mellitus cases: Obesity, fueled by the high-fat American diet readily available at McDonald’s and other fast-food restaurants nationwide.
There seems to be a medical consensus on this: Physicians routinely fault the Golden Arches and its ilk for our widening waistlines. See my 5/12/16 Tidbit, on this website, for follow-up comments by Dr. Bernhard Liese, chairman of the Georgetown University Dept. of International Health. The number of obese people worldwide, Liese said, has doubled since 1980. Not coincidentally, McDonald’s spread has expanded globally.
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDKD), over two-thirds of all adult Americans (68.8%)—roughly 160 million people—are overweight, and over one-third (35.7%) are obese. The World Health Organization defines overweight as a body-mass index (BMI) between 25 and 29.9 and obesity as a BMI of 30 and above. BMI is your weight in kilograms divided by the square of your height in meters.
I’m talking fat here because I believe it’s vitally important to think of Type 2 DM, which typically begins in middle age—a physiological time when the body’s lean-muscle mass declines and fat mass increases (see my book!)—as a consequence of too much fat.
While Type 2 DM can develop in thin people, too, it commonly does so only in thin elderly people. For the vast majority of people—for the one in three Americans who have “prediabetes,” as I defined it on my Facebook page and again below—the problem is fat, especially visceral fat, which is stored within the abdominal cavity and, thus, around the liver, the pancreas, and the intestines.
Don’t let fat beat you.
**
GLUCOSE AND INSULIN
As I explained on Facebook, glucose is our bodies’ primary energy source. We get glucose, which is a monosaccharide, from the carbohydrates that we eat. You probably have heard about athletes loading up on carbs, typically by eating pasta, before marathons and other sporting events. They’re obtaining mega-energy.
Once consumed, carbohydrates pass from our stomachs into our small intestines, where they are broken down into glucose. Our bodies convert some of the glucose into glycogen, which is stored in our livers (and, therefore, at the ready, to be converted into glucose again) and our muscles. The remaining glucose enters the blood through the liver and the gastrointestinal tract and travels to cells and organs to fuel them. As I mentioned on Facebook, the brain is exclusively dependent on glucose for functioning.
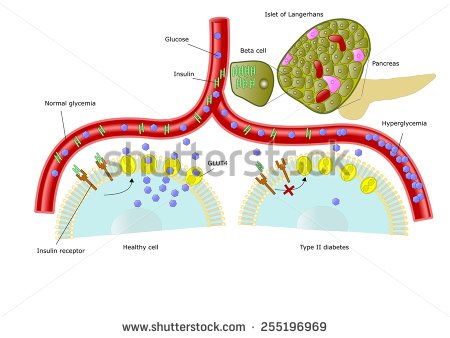
The hormone insulin helps our bodies absorb glucose and use it for energy. Specialized beta cells of the pancreas, a gland that sits behind the stomach, produce insulin in the amount needed to move glucose into our cells, where it is stored and used later. Insulin is the “key” that unlocks the doors that glucose travels through to get into our bodies’ cells. If this sugar cannot enter the cells, an abnormally high level of it can build up in the blood, creating a condition called hyperglycemia. Chronic hyperglycemia is diabetes (I am grossly over-simplifying the biochemistry involved in glucose metabolism.)
TYPES OF DIABETES
As you undoubtedly know, there are two main types of diabetes. People with Type 1 diabetes mellitus, also known as insulin-dependent diabetes, cannot make enough insulin to transport glucose. This is because their bodies’ immune systems have destroyed most of their pancreatic beta cells. According to Dr. Clement, by the time Type 1 DM clinically manifests, only 10 percent of the beta cells remain. The first-line treatment for Type 1 diabetes, therefore, is the introduction of insulin into the body, either through injection or by an insulin pump. Insulin cannot be taken orally.
In contrast, Type 2 diabetes, which constitutes 90 to 95 percent of all DM diagnoses, occurs because of “multiple defects,” physicians say, including decreased insulin secretion (but not an absence of production), so-called insulin resistance, and hepatic glucose overproduction (the liver is producing too much glucose).
People who develop Type 2 diabetes can make insulin, but they either don’t make enough of it, because of beta-cell dysfunction, and/or “their fat, liver, and muscle cells do not respond correctly to [their] insulin,” according to the online National Library of Medicine. The cells’ improper response, their disregard of the insulin, is called insulin resistance.
More specifically, according to Dr. Clement, insulin resistance is “an acquired abnormality related to an accumulation of visceral adipose tissue” in people “genetically predisposed” to diabetes. Visceral fat, which is intra-abdominal fat that you cannot feel, releases substrates, such as free fatty acids, or hormones that impair insulin action, he explained. (Elsewhere, I read that visceral fat secretes a protein that increases insulin resistance.)
People with insulin resistance need more insulin to help glucose enter their bodies’ cells. At first, their pancreases will compensate by producing enough insulin to meet the new demand, but, over time, they will lose their ability to produce more, and blood-glucose levels will rise.
On Facebook, I defined a diagnosis of Type 2 diabetes as a fasting plasma glucose level of 126 mg/dL (milligrams per deciliter) or more. You also may see a diagnosis based on an oral glucose tolerance test: If your blood-sugar level is higher than 200 mg/dL two hours after you’ve drunk a special sugar drink, you’re considered diabetic. It’s wise to repeat whichever test you take to confirm the result. (A third test based on hemoglobin is also available.)
When glucose builds up in your blood, your cells may become starved for energy, says the American Diabetes Assn. Over time, the high sugar concentration can damage your eyes (resulting in vision impairment), kidneys (leading to dialysis or the need for a kidney transplant), nerves (causing pain, tingling, and numbness; digestion or urination problems), and/or heart (weakening it). Most diabetics die from heart disease.
Because of nerve and blood-vessel damage, Type 2 diabetics usually have foot problems. It becomes harder for their blood to flow to their legs and feet; sores and infection may develop in these extremities, necessitating amputation.
People with Type 2 DM often have no symptoms initially or even for many years. Early symptoms include:
*Bladder, kidney, skin, or other infections that occur frequently or are slow to heal
*Fatigue
*Increased hunger
*Increased thirst
*Increased urination
*Blurred vision
*Numbness or tingling in the feet or hands
*Unexplained weight loss
Another type of diabetes called secondary diabetes mellitus may result from an underlying medical problem or as an adverse effect of certain medications, including thiazide diuretics and beta blockers, used to treat hypertension; steroids; and oral contraceptives. Treatment of this DM would depend on the cause.
**
RISKS AND PREVENTION
You are more likely to develop Type 2 diabetes if you:
*Are 45 years old or older
*Are overweight, meaning your BMI is 25 kg/m2 or greater (poor diet goes along with this)
*Have a family history of diabetes mellitus in a first-degree relative (parent, sibling)
*Are habitually physically inactive
*Are a member of a high-risk ethnic or racial group, including African-Americans, Latinos, Native Americans, Asian-Americans, and Pacific-Islanders
*Have a history of delivering a baby weighing more than 9 lbs., or of gestational diabetes
*Have a blood-sugar level between 100 and 126 mg/dL (prediabetes)
*Have blood pressure over 140/90 mmHg
*Have cholesterol levels higher than normal (HDL (good cholesterol) below 35; blood triglyceride level above 250)
*Have polycystic ovary syndrome
*Have a history of cardiovascular disease
Excess visceral fat has not yet made the standard list of risks for Type 2 DM. According to the NIDDK, however, a waist measurement of 40 inches or more for men and 35 inches or more for women is associated with insulin resistance and increases a person’s risk for Type 2 DM. This is true even if your BMI is normal.
In the Diabetes Prevention Program, a recent federally funded study of 3,234 people at high risk for diabetes, the strongest risk factors for Type 2 diabetes proved to be higher-than-normal blood-sugar levels, obesity, and a family history. Half of the participants came from minority groups with high rates.
The good news from the DPP and other studies is that losing weight, eating healthier (reducing fat and calorie intake), and being more physically active can prevent or delay the development of Type 2 diabetes. The NIDDK says that “every pound you lose lowers your risk of getting diabetes.” If you’re in the high-risk group, your goals should be 1) to reach and maintain a reasonable body weight; 2) to make smart food choices most of the time (fruits, vegetables, whole grains, fish, lean meats); and 3) to be physically active every day.
(Physicians recommend the DASH diet, which is based on the Mediterranean diet. I cover this diet in detail in my book.)
There are many medications available to control blood-sugar levels, but they are not without their complications. An analysis published in the April 19, 2016 issue of “The Annals of Internal Medicine” concluded that metformin, the most frequently prescribed “standalone” drug for Type 2 DM, is better for your heart than its closest competitors. Some researchers believe that metformin, which has been in use since the late 1990s and is now a generic drug, is the safest and more effective Type 2 DM medication available; others endorse pioglitazone (Actos), empagliflozin (Jardiance), and liraglutide (Victoza). This is a decision you obviously must make with your doctor. Do your drug-risk homework before you take any medication.
The DPP used three subject groups to test three approaches for preventing Type 2 DM. The first group only made lifestyle changes, usually by walking five days a week for 30 minutes and lowering fat and calorie intake. The second group took metformin and made no lifestyle changes. The third group received education about physical activity and diet, but took no medication. People in the lifestyle-change group showed the best outcomes, but the metformin group benefited, too.
Diabetes is a lifelong disease; there is no cure. But some people with Type 2 DM no longer need medication if they lose weight and become more active. When they reach their ideal weight, their body’s own insulin and a healthy diet can control blood sugar.
I’m a big believer in exercise as the best magic pill we have for aging well. Exercise will:
*Lower your blood-sugar level without having to resort to medication
*Burn extra calories and fat
*Improve your blood flow and blood pressure
*Increase your energy level
*Improve your ability to handle stress
*Mobilize your visceral fat (according to Dr. Clement)
I highly recommend the NIDDK’s publication, “Am I at Risk for Type 2 Diabetes? Taking Steps to Lower Your Risk of Getting Diabetes,” available at http://www.niddk.nih.gov/health-information/health-topics/Diabetes/type-2-diabetes-taking-steps-lower-your-risk-diabetes/Pages/index.aspx for more information.
The NIDDK has provided tables that enable you to calculate your BMI with weight in pounds and height in inches.
Ann, 5/26/16
