(PLEASE NOTE: Much of the content below was excerpted from “The Aging Body” chapter of my book, “Our Parents in Crisis,” in which I highlight the normal physiological changes that occur with aging in every system of the body.)
Your skin undergoes genetically determined intrinsic aging, aka chronological aging, as well as extrinsic aging, caused by environmental factors such as the sun’s ultraviolet (UV) radiation, cigarette smoke, harsh weather, and even pollution. (1)
That’s the bad news.
The good news is if you avoid environmental influences, especially UV exposure, you can generally preserve your skin’s smooth and unblemished appearance, as my 92-year-old mother has.
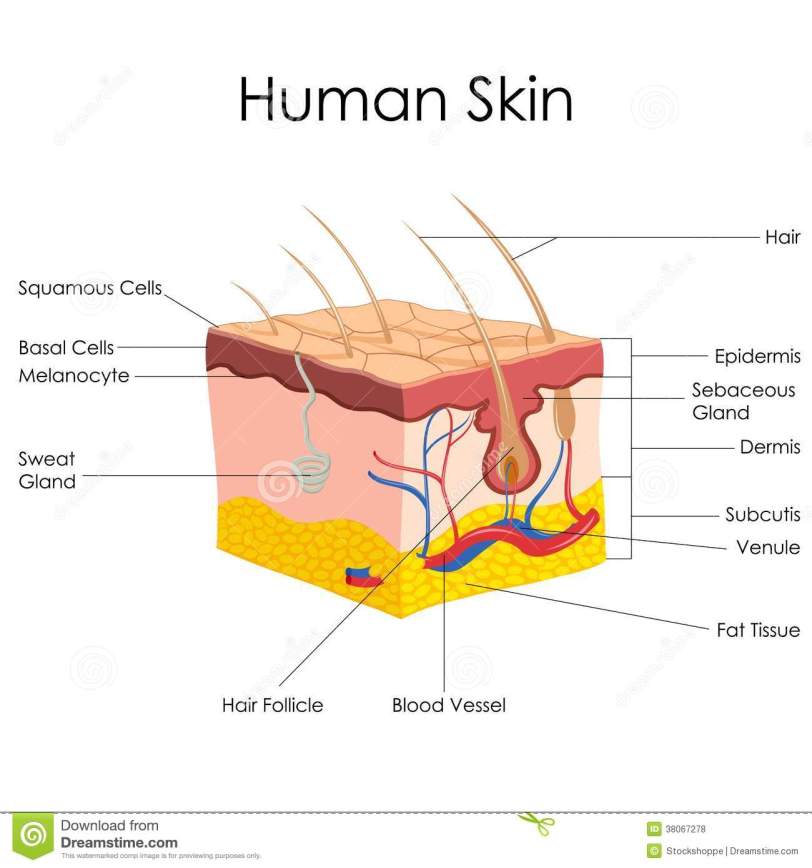
Skin is part of the integumentary system—an integument being an outer covering—which also includes the hair, the nails, and the oil, sweat, and mammary glands. It is the largest organ in the body.*
The skin consists of three main layers: the epidermis (including the visible skin); the dermis; and the subcutaneous tissue (aka hypodermis). Intrinsic aging causes structural and functional changes in all of these layers.
THINNING OF SKIN, LOST PROTECTION
Because of the abuse skin takes from the sun and other environmental elements, epidermal cells must be continuously replaced, a process that takes about 28 days in young skin. The new, fresh cells come up from the subcutaneous layers. Between the ages of 30 to 80, the turnover rate of skin-cell replacement slows about 30 to 50 percent. This slower turnover causes thinning of the epidermis—giving it a translucent look, like frosted glass—and diminishes the skin’s repair and cell exfoliation. Corneocytes, which aid in the skin’s barrier function, tend to clump together on the surface of aged skin, creating a rough, scaly appearance and texture.
Melanocytes are epidermal cells that provide protective melanin pigment. With age, their number declines, as does the functional activity of the remaining melanocytes. This reduction leads to thinner, paler, and more translucent skin, as well as color changes such as mottled pigmentation and freckles. The decline of melanocytes also reduces your skin’s protective capacity against UV radiation.
The dark spots or hyperpigmentation that you may see on older white skin—especially in Florida—is caused by erratic melanocyte activity brought on by long-term sun exposure, not by a reduction of melanocytes.
The number of Langerhans cells, which are immunocompetent epidermal cells similar to melanocytes, also decreases—by nearly 50 percent in the very old. The loss of these cells compromises the skin’s immune surveillance and leads to a higher risk of skin cancer. The longer sun exposure that older epidermal cells have because of slow turnover time also increases your Mom’s or Pop’s cancer risk.
A prominent change occurs with age at the junction between the dermis and the epidermis. The normally undulated membrane that separates these two layers flattens out, decreasing the transfer of nutrients between the layers and diminishing the renewal and healing of older skin.
During the aging process, the dermis can lose from 20 to 80 percent of its thickness. This is because of changes in collagen, elastin, and other protein biosynthesis. Loss of sebaceous glands in this layer also makes older skin drier.
The age-related degradation of collagen and elastin, two important constituents of bone and other body parts, has widespread implications beyond just skin.
Collagen is a fibrous protein. My father, who studied collagen and what were called connective-tissue diseases in the 1960s, once explained it to me as follows: “Collagen makes up your connective tissues—your tendons, cartilage, ligaments, what have you—and holds together anything that is tied together, except the brain itself: the bone, the blood vessels, the heart, the lungs, the intestinal tract. If you didn’t have collagen, you’d just fall apart. You’d be a little blob on the floor.”
You can’t beat blob imagery for capturing functional essence. Collagen figures prominently in growth and also plays a role in the healing of wounds, scarring, and the pathogenesis of diseases, as well as aging.
As a person ages, more and more “cross links” form between adjacent collagen molecules, and they bind together “like rungs in a ladder,” according to Dr. Al. Strands of cross-linked collagen polypeptides tend to be more fibrous, and, thus, harder and less flexible.
The lens of the eye is one of the first structures to exhibit age-related changes as a result of increased collagen rigidity. Because of this rigidity, most people age 55 and older need reading glasses. But cross-linking also affects tissues in the heart, lungs, kidneys, and joints, greatly reducing their functional ability.
Elastin is a protein that accounts for elastic fibers in tissue. Wherever elasticity occurs, such as in the lungs, the bladder, the major arteries of the heart, and the skin, fibers containing elastin exist. Like collagen, elastin and elasticity decline with age.
As skin thins, bruising occurs more easily, and bruises heal more slowly. Also with age, the dermal microvasculature (blood vessels) becomes more fragile and subject to rupture. Not only do you lose vessels, thus reducing your skin’s blood supply, but you lose the fatty subdermal layer that helps to protect vessels from injury. The loss of this padding leads to wrinkling and sagging of the skin and increases its susceptibility to trauma and bruising.
If your Mom or Pop takes an anticoagulant or aspirin, bleeding from capillary damage may take longer to stop and cause severe bruising. A diminished blood flow—perhaps caused by narrowed arteries—can further impair wound healing. If you see large, ghastly, discolored bruises on your Mom’s arms or legs, don’t panic. Given a plausible reason for the wound, allow it time to heal.
Because of the age-related decline in the density of the dermal blood supply, which provides oxygen and nutrients to the tissues and an efficient means by which to regulate body temperature, elders become more vulnerable to sunburn. This decreased density, coupled with a gradual loss of functioning sweat glands, predisposes your Mom and Pop to heat stroke. (2)
When many of us think of aged skin, we think of wrinkles, of which there are two types: Intrinsically aged wrinkles occur as a result of a reduction in muscle mass and skin thickness (normal changes); cross-linking of collagen and elastin in the dermis; and dehydration in the epidermis. These are typically either “fine” wrinkles or expression lines. Extrinsically aged wrinkles, such as those on the face and chest, are deeper, coarser, and more numerous.
Sun-induced photoaging is the chief perpetrator of your skin’s extrinsic aging. Besides wrinkling, photoaging causes yellowing, irregular pigmentation, and the benign dermatologic lesions that we call “age” or “liver” spots, as well as other blemishes that multiply over time. Although most of the sun’s damage to a person’s skin occurs before age 65, geriatricians still advise elders to wear sunscreen. I wear it year-round.
Cigarette smoking also can severely age the skin, creating hard wrinkles and irregular splotches. This self-destructive habit can add 10 to 15 years to a smoker’s facial appearance.
Ann, 6/15/16
*Most of the available clinical data pertain to Caucasian skin, not black skin, which contains more protective melanin pigment.
Endnotes:
1. Dermatologists at the University of California-Irvine medical school provide an excellent review of skin aging in Jerry L. McCullough and Kristen M. Kelly, “Prevention and Treatment of Skin Aging,” Annals of the New York Academy of Sciences 1067 (2006): 323-31. Changes caused by chronological, as opposed to environmental aging, are ibid, 323-24.
2. David A. Sandmire, pp. 69-70 in Gerontology for the Health Care Professional, ed. Regula H. Robnett and Walter C. Chop (Sudbury, Mass.: Jones and Bartlett Publishers, 2nd ed., 2010 ).
