
Only about 13 to 15 percent of all strokes suffered by people are hemorrhagic strokes like the one that the Los Angeles County coroner has determined caused the death of show-business legend Debbie Reynolds, 84, last month.
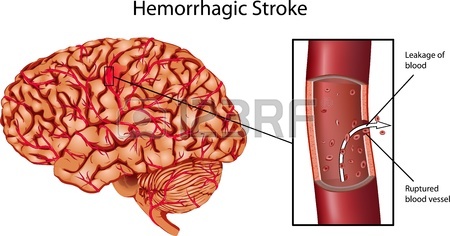
Hemorrhagic strokes typically occur when an aneurysm, which is a balloon-like bulge or swelling in the wall of a cerebral artery, ruptures, so there is bleeding in the brain. (An aneurysm can occur in other arteries outside of the brain, too.) The weakened wall gives way, usually because of the force of blood pushing against it as the heart pumps. The higher the blood pressure in a vulnerable artery, therefore, the greater the risk of a hemorrhagic stroke.
This is what happened to Reynolds. She had an intracerebral (within the brain) hemorrhage, brought on by what the coroner described as dangerous hypertension (high blood pressure). Emotional stress may have played a part in the timing of Reynolds’s stroke, inasmuch as she was stricken a day after her beloved daughter Carrie Fisher’s sudden death.
***
Hemorrhagic vs. Ischemic
Bleeding from a ruptured brain aneurysm—or even just a blood leak, not a full rupture—causes swelling of the brain and increased pressure in the skull. Swelling and pressure, in turn, cause damage to brain cells and tissues; this damage is called a stroke.
Hemorrhagic strokes also may be subarachnoid, meaning that the blood vessel that bursts is outside of the brain, so that bleeding occurs in the subarachnoid space between the brain and the tissues covering it. Cerebral spinal fluid circulates in this space.
An ischemic stroke is far more common than a hemorrhagic stroke (85-87 percent of total). This type of stroke occurs when the blood flow within a cerebral artery is blocked or obstructed, typically by a clot.
A clot-induced ischemic stroke may be either thrombotic or embolic. In a thrombotic stroke, a blood clot forms in an artery that supplies blood to the brain. In an embolic stroke, a blood clot or other substance, such as “plaque,” travels from another location—such as the heart—through the bloodstream to an artery in the brain, where it obstructs blood flow. Within four minutes of being deprived of the oxygen that arterial blood supplies, brain cells begin to die. (1)
(Atrial fibrillation is a common cause of embolic strokes because the blood moves slower and tends to pool in the heart with this arrhythmia, thereby increasing the risk of blood clots forming. People with AF often take an anticoagulant, such as warfarin (Coumadin), to prevent clot formation.)
According to Dr. Victor C. Urrutia, a neurologist and director of the Johns Hopkins Hospital Stroke Center, 20 percent of all ischemic strokes are caused by atherosclerotic cerebrovascular disease. (2) Atherosclerotic blood vessels have walls thickened by fatty material that is collectively known as plaque. These fatty deposits narrow the lumens (canals) of vessels, thereby restricting blood flow. Carotid artery disease, which is a buildup of plaque in the two big arteries (the carotids) in the neck that supply blood to the brain, causes many ischemic strokes.
The effects of a stroke vary from person to person and depend on its type, severity, and location. Classic stroke symptoms include slurred speech, paralysis or numbness on one side of the body or face (causing a droop), blurred vision, mental confusion, a severe out-of-the-blue headache (the worst of your life, says Dr. Urrutia), dizziness, and a loss of balance.
A stroke may impair a person’s movement and sensation, speech and language, vision, cognition (reasoning, memory), perception, emotional control, bowel and bladder control, and other vital body functions. A stroke can cause permanent brain damage, long-term disability, or death.
A transient ischemic attack (TIA), or so-called mini-stroke, produces symptoms similar to a stroke, but usually only lasts a few minutes and causes no permanent damage. With a TIA, blood flow is only temporarily disrupted. A TIA may be a warning of an impending stroke, however, and should not be ignored.
***
THINK FAST: Time is of the Essence
During a stroke, every minute counts. The longer a stroke goes untreated, the greater the potential is for damage. Prompt medical and/or surgical treatment can reduce brain damage, prevent permanent disability, and save life.
The Mayo Clinic has an easy-to-remember acronym for helping a loved one, friend, or acquaintance to decide when to seek immediate medical treatment for someone who may be having a stroke: Think FAST:
(F)ACE: Ask the person to smile. Does one side of the face droop?
(A)RMS: Ask the person to raise both arms. Does one arm drift downward? Or is it impossible for the person to raise one arm?
(S)PEECH: Ask the person to repeat a simple phrase. Is his/her speech slurred or strange?
(T)IME: If you observe any of these signs, call 911 immediately.
Stroke has long been the second or third leading cause of death in the United States. Don’t second-guess yourself about stroke symptoms. If you do, you’ll waste precious time. Make the call.
Tissue plasminogen activator (tPA), a drug that functions as a clot dissolver or clot buster, has been the mainstay treatment during the past 20 years for a person who has had an ischemic stroke. For tPA to be effective, however, it must be given intravenously within four and a half hours of the onset of symptoms—and preferably, within three hours. The sooner, the better. According to Dr. Urrutia, tPA substantially reduces the likelihood of long-term disability or death.
Ischemic-stroke patients who cannot take tPA, for medical reasons, may be given an antiplatelet medication, to stop their platelets from clumping to form more blood clots, or an anticoagulant, such as aspirin or warfarin, to prevent existing blood clots from growing larger.
Tissue plasminogen activator aggravates cerebral bleeding, however, so it should not be given to hemorrhagic stroke patients like Reynolds. A brain computed tomography (CT) scan or an MRI of the brain or both can be used to diagnose a stroke, discover its cause, and pinpoint the location of the bleeding or brain-cell damage.
A physician may prescribe medication to lower the blood pressure of a person who has suffered a hemorrhagic stroke. He or she also may perform surgery to “clip” the aneurysm with a tiny clamp to prevent further blood leakage or to insert a tiny coil into the aneurysm to cause a blood clot to form and block any more blood flow through it. These procedures are known, respectively, as an aneurysm clipping and coil embolization.
If an arteriovenous malformation (AVM) is the cause of the hemorrhagic stroke—“AVM is a tangle of faulty arteries and veins that can rupture within the brain,” according to the National Heart, Lung, and Blood Institute)—the physician may try to repair the AVM to prevent further bleeding. This is a rare form of hemorrhagic stroke.
***
Mechanical Thrombectomy
Because tPA often does not completely dissolve large blood clots in larger blocked arteries, it may be necessary for a physician to remove the clot itself. Such surgery is known as a mechanical thrombectomy. Since 2004, the U.S. Food and Drug Administration has approved three different classes of devices for mechanical thrombectomy, the latest (2012) being a stent retriever.
To ensure effectiveness, a mechanical thrombectomy should be performed within six hours of the presentation of acute stroke symptoms and ONLY after the patient has received tPA. A stent retriever is a wire cage that a physician delivers to the blocked cerebral artery in a catheter tube that he/she threads through an artery in the groin up to the brain. The stent opens and grabs the clot, and the physician removes it with the trapped clot. Special suction tubes also may be used.
To be confident of access to tPA, of tPA’s proper use by physicians, and of the availability of mechanical thrombectomy, you or the patient for whom you’re advocating should go to a university-affiliated or other known stroke center. That is the reality of our health-care system.
Consider the following anecdote published online by the American Heart Association in an article about stent retrievers:
“Two days before Christmas in 2012, Donald Sadoway and his wife were having lunch with friends when someone proposed a toast, and he didn’t respond.
“‘I just stared at the glass,’ said Sadoway, 65, a chemistry professor at Massachusetts Institute of Technology who earlier that year had been named one of Time’s 100 most influential people.
“Sadoway couldn’t speak, and then his right side collapsed. An ambulance arrived within minutes and took Sadoway to nearby Massachusetts General Hospital [which is affiliated with Harvard Medical School].
“Sadoway received tPA 16 minutes after stroke symptoms started. Within the hour, doctors were pulling the 4-millimeter clot from his brain.
“‘No more than two hours after the procedure, I’m sitting up in recovery and talking to my kids,’ said Sadoway, who has made a complete recovery except for some minor problems with fine motor skills.”
To me, this is nothing short of amazing. If you’re going to have a stroke, it’s best to have it near the Mass General, Johns Hopkins, the Mayo Clinic, Stanford, the University of Chicago, Duke . . . you get my point.
For an excellent overview of strokes, their causes, treatments, and prevention, see the National Heart, Lung, and Blood Institute at https://www.nhlbi.nih.gov/health/health-topics/topics/stroke.
Atherosclerosis is a root cause of many strokes. I’ll take a look at this common chronic vascular condition in my next blog.
Ann, 1/14/17
1. Dr. Alexander W. Dromerick, “Under Pressure: Understanding How High Blood Pressure Affects Your Health,” presented by the Georgetown Center for Hypertension, Kidney & Vascular Research at the Georgetown University Medical Center, March 31, 2012.
2. Dr. Victor C. Urrutia, “Stroke Essentials,” presented in Johns Hopkins Medicine’s “A Woman’s Journey” conference, Baltimore, Md., Nov. 17, 2012. According to Urrutia, 20 percent of ischemic strokes are caused by atherosclerotic cerebrovascular disease, and 20 percent are caused by blood clots. Of the remaining 60 percent, Urrutia said 30 percent of strokes are cryptogenic, meaning their cause is not known, and 25 percent are lacunar, meaning another defect is responsible. He has a 5-percent margin of error.
