Georgetown University opened the spring semester of its outstanding Mini-Medical School program last Tuesday with a fact-filled lecture about traumatic brain injury (TBI) by Mark Burns, Ph.D., an associate professor in the medical school’s neuroscience department. Dr. Burns’s research focuses on the link between TBI and Alzheimer’s disease.
A good-natured Irishman (Happy St. Patrick’s Day), Dr. Burns has been a busy speaker this month which, unbeknownst to me until I started writing this blog, is Brain Injury Awareness Month. Tuesday, March 20, is Brain Injury Awareness Day on Capitol Hill. For details about the day’s events, see https://www.biausa.org/public-affairs/public-awareness/news/brain-injury-awareness-day-is-march-20-2018.
Dr. Burns gave a lively and—considering the complexity of his subject—commendable overview in just under two hours. After his talk, I did a TBI crash course of my own in order to fill in some gaps. I will endeavor to do Brain Injury Awareness Month and Day justice in the highlights below.
***
What is Traumatic Brain Injury?
A traumatic brain injury occurs whenever the brain is wounded by a penetrating object, such as a bullet, shrapnel, knife, or other weapon, or by a non-penetrating external physical force such as a bump, blow, or jolt to the head. A person can suffer both penetrating and non-penetrating TBIs, dual injuries that are typically associated with an explosion, a natural disaster, or other extreme event.
A traumatic brain injury is caused by two mechanisms: impact and movement of the brain within the skull. The brain’s two cerebral hemispheres are not fixed rigidly inside the skull and have a lot of room in which to move. In either case, mechanical forces compress or lacerate the brain’s surface and create shock waves that travel through it and injure parts remote from the impact site.
Before I go further, I think it’s helpful to review some brain anatomy and other physical facts, which Dr. Burns did not do. It’s easy to get lost without an anatomical and physiological frame of reference.
The jello-like brain is the main processor or command/control center in the vertebrate central nervous system, which also consists of the spinal cord. It weighs about 3 pounds and is the fattiest organ in the body. Your brain sends signals to your body through your nervous and endocrine systems, which are interconnected, but distinct: Impulses from the nervous system travel rapidly–in milliseconds–by electrochemical means, while the endocrine system releases chemicals (hormones) that act upon their targets in speeds varying from seconds to hours.
The cerebrum accounts for about 85 percent of the brain’s weight and consists of the two cerebral hemispheres, left and right, each of which has a cerebral cortex, as well as some subcortical (beneath the cortex) structures such as the hippocampus.
The brain stem lies underneath the cerebrum and connects to the spinal cord. Parts of the brain stem control and regulate vital body functions, such as respiration, heart rate, and blood pressure. The stem parts are critical to the regulation of involuntary functions.
Behind the brain stem sits the cerebellum, which appears to be a separate structure from the “big” brain. Indeed, cerebellum is Latin for “little brain.” The little brain chiefly affects motor control, playing a role in coordination and balance, but it also may have some cognitive functions.
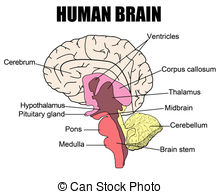
The cerebral cortex, which is the outermost layer of the cerebrum, is divided into four lobes, the frontal, temporal, occipital, and parietal. I will not delve into the neurological functioning of each lobe. Suffice it to say that the cortex controls your cognitive everything: your reason, your memory, your sensory integration, your planning, your language, your attention, your spatial sense, etc., etc. Higher-level functions such as self-control, logic, and abstract thought are associated with the frontal lobes.
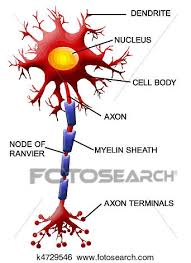
The basic electric unit of the brain is the neuron, also known as the nerve or nerve cell. The brain has about 86 billion to 100 billion neurons (depending on which source you believe), which have three components: a cell body, an axon, and a dendrite. Generally speaking, the brain’s gray matter consists of the nerve cell bodies. Its white matter consists of the axons that carry electrical impulses away from nerve cell bodies, and the dendrites that carry signals to the cells. Axons are long projections sheathed in myelin, a fatty protective coating.
The brain is made up of 40 percent gray matter and 60 percent white matter.
The brain is also 75 percent water. Water is the chief constituent of cerebrospinal fluid (CSF), which is an intracellular fluid that flows around and inside the brain and spinal cord. Among its many functions, CSF protects brain tissue from injury when it is jolted or hit by acting as a fluid buffer or shock absorber.
***
The Damage Range of TBIs
Traumatic brain injuries range from mild, in which a brief change in mental status or consciousness occurs, to severe, in which an extended period of unconsciousness or amnesia ensues.
TBI-related damage can be confined to one area of the brain, in which case it is known as a focal injury—an example being a localized insult, such as a contusion (bruise)—or it can occur over a more widespread area, which is known as a diffuse injury. The area of the brain that is injured determines both the injury’s symptoms and the impairment and disability it causes.
A diffuse axonal injury (DAI) is one of the most common types of TBI. DAI refers to widespread damage to the brain’s white matter, i.e., to bundles of axons.
DAI is the result of shearing forces, which stretch or tear axon bundles. Such injuries most commonly occur as a result of auto accidents, sports injuries, or falls, when the brain is violently in motion. (Think of whiplash.)
Unfortunately, Dr. Burns explained, damage from a DAI is not obviously visible on a brain scan. With a DAI, there’s no obvious bleeding or contusion. A shearing injury results instead, he said, in “broken connections” among nerve cells, disrupting neural circuits, and causing an overall communication breakdown.
DAIs can cause temporary or permanent damage to the brain, and recovery can be prolonged.
Because a severe TBI is evident to anyone who attends the patient, Dr. Burns focused in his talk on mild TBIs, which have the potential to rapidly become serious, even fatal, if neglected. I will do the same, except to note that the immediate goal of treatment for the person who has suffered a severe TBI is to prevent death.
The severe TBI person’s spinal cord, heart, lung, and other organ functions must be stabilized, and further brain damage must be prevented. Persons with severe TBI generally require a breathing machine to ensure both respiration and proper oxygen delivery. They may need surgery to relieve pressure inside the skull, to get rid of damaged or dead brain tissue, or to remove hematomas. I’ll look at pressure and hematomas below.
***
The First 24 Hours
The first 24 hours after a mild TBI are particularly important because hematomas (pooling of blood in the tissues outside of the blood vessels), contusions (bruising), and excessive brain swelling (edema) are possible and can cause further secondary damage.
This is what happened to actress Natasha Richardson, who suffered a head injury while skiing, but who declined medical assistance because she felt fine. A few hours after her fall, she suffered a debilitating headache. A massive epidural hematoma eventually led to her death.
Hematoma describes swelling in the brain when a blood vessel breaks. Hematomas are characterized by where the blood collects relative to the brain’s protective membranes, which are called meninges. The meninges have three layers: dura mater (outermost); arachnoid mater (middle), and pia mater (innermost). There are three types of hematomas:
Epidural hematoma: involves bleeding into the area between the skull and the dura mater. Such a bleed can occur with a delay of minutes to hours after a skull fracture damages an artery under the skull, and are particularly dangerous.
Subdural hematoma: involves bleeding between the dura and the arachnoid mater and, like an epidural hematoma, exerts pressure on the outside of the brain. Their effects vary depending on their size and the extent to which they compress the brain. Subdural hematomas are very common in elderly people after a fall.
Subarachnoid hematoma or hemorrhage: involves bleeding between the arachnoid mater and the pia mater. Their effects vary depending on the amount of bleeding.
Bleeding into the brain itself is called an intracerebral hematoma. This bleed damages the surrounding tissue.
(The material above is courtesy of the National Institute of Neurological Disorders and Stroke (NINDS), whose website I consulted after Dr. Burns’s talk.)
The primary or immediate effects of a mild TBI on the brain can include “various types of bleeding and tearing forces that injure nerve fibers and cause inflammation, metabolic changes, and brain swelling,” according to the NINDS.
Secondary consequences of TBI manifest gradually over the course of hours, days, or weeks, and are the result of reactive processes that occur after the initial head trauma.
For example, if an initial contusion—which is a bruising or swelling that occurs when very small blood vessels bleed into the brain—continues to bleed and expands over time, this “hemorrhagic progression” will create a new or larger lesion, i.e., damage to more tissue.
“This increased exposure to blood, which is toxic to brain cells,” the NINDS explains, “leads to swelling and further brain cell loss.”
When the brain sustains a powerful blow, swelling occurs just as it would in other parts of your body. The problem with brain edema is that the skull cannot expand. When brain tissue swells, the pressure inside the skull rises. This pressure is called intracranial pressure (ICP) and is measured in millimeters of mercury, just like blood pressure is. If intracranial pressure becomes too high, it prevents blood from flowing to the brain, thus depriving it of oxygen. Oxygen deprivation can permanently damage brain function.
According to Dr. Burns, the most common cause of death in the ICU after a traumatic brain injury is intracranial pressure.
Normal ICP is between 7 and 15 mm Hg. Dr. Burns defined intracranial hypertension as a pressure of more than 20 mm Hg. A pressure of more than 40 mm Hg will cause impairment of electrical activity; a pressure of more than 60 mm Hg is fatal.
A breakdown in the blood-brain barrier, which preserves the separation between the brain’s fluid and the capillaries that bring the brain oxygen and nutrients through the blood, also can cause secondary damage.
***
Signs and Symptoms of TBI
During an initial evaluation after a mild TBI, subtle functional and cognitive difficulties can go undetected and may not emerge until days later. According to the NINDS, headache, dizziness, confusion, and fatigue tend to start immediately after an injury, but resolve over time. Emotional symptoms such as frustration and irritability tend to develop later on during the recovery period. Many symptoms overlap with other conditions, such as depression or sleep disorders.
The NINDS advises people to seek immediate medical attention if they experience any of the following symptoms:
*loss of, or change in, consciousness, anywhere from a few seconds to a few hours
*decreased level of consciousness
*convulsions or seizures
*unequal dilation in the pupils or double vision
*clear fluids draining from the nose or ears
*nausea and vomiting
*new neurologic deficit, such as slurred speech, weakness of arms, legs, or face, or loss of balance
As noted above, secondary damage is the reason that doctors advise watching a person for cognitive and other changes for 24 hours after an injury. The common symptoms that need monitoring, the NINDS says, include:
*mild to profound confusion or disorientation
*problems remembering, concentrating, or making decisions
*headache
*light-headedness, dizziness, vertigo, or loss of balance or coordination
*sensory problems, such as blurred vision, “seeing stars,” ringing in the ears, bad taste in the mouth
*sensitivity to light or sound
*mood changes or swings, agitation (feeling sad or angry for no reason), combativeness, or other unusual behavior
*feelings of depression or anxiety
*fatigues or drowsiness, a lack of energy or motivation
*changes in sleep patterns; inability to wake up from sleep
I once fell on black ice and hit my head on street blacktop. I did not lose consciousness, nor did I have a headache or experience any dizziness. I just felt jolted, shaken.
Fearing a hematoma, I monitored myself as best as I could and only breathed a sign of relief after days had passed. For more than a month, however, I felt emotionally blunted, as if my brain were wrapped in plastic and I couldn’t experience the world as it truly was. I felt what people call the Teflon effect: Nothing stuck to me. I was profoundly detached from my environment.
The advantage to my Teflon state was that I also felt serene and peaceful. Because nothing “stuck” to me, I had no worries. I didn’t even worry about my altered state of mind. I just waited it out.
I always wondered if my change in consciousness and outlook might have been a “slight” concussion. Dr. Burns defined a concussion as a brain injury that typically results in “the rapid onset of short-lived impairment of neurological function that resolves spontaneously.”
This Tuesday, I will return to the subject of traumatic brain injury and discuss concussions, including chronic traumatic encephalopathy (CTE), which develops with repeated blows to the head, such as those football players suffer, and comas.
Please come back for my TBI continuation.
Ann, 3/17/18
